

Melasma Case Study: A Personalised Clinical Approach to Pigmentation at AMRÉ
Melasma is one of those skin concerns that can feel particularly frustrating to navigate. Not because it is rare, but because it rarely responds to a one-size-fits-all approach. It is a chronic pigmentary condition that presents as symmetrical brown or grey-brown patches, most commonly across the cheeks, chin, upper lip, and forehead. What makes it so persistent is that it is rarely caused by just one thing. UV exposure, hormonal shifts, genetic predisposition, and oxidative stress all contribute, often simultaneously

At AMRÉ, I approach melasma the way I approach most things: by looking at the whole picture. In this case, that meant building a protocol that combined a structured, medical-grade skincare regimen with targeted naturopathic vitamin therapy. The goal was not only to address what is visible on the surface, but to understand and support what is driving it from within. This is the clinical journey of one of our patients over an eight-week period.
Patient Presentation
Before any treatment begins, I make it a priority to understand the full picture of who I am working with. Melasma does not present the same way in every patient, and what works beautifully for one person may not be appropriate for another. A thorough assessment at the outset saves time and prevents unnecessary frustration.
Demographic Context
Age Range: Early 50s
Skin Type: Fitzpatrick Type IV
Duration of Concern: Approximately 18 to 24 months of progressive pigment change
Primary Concern: Bilateral facial hyperpigmentation consistent with melasma
Presenting Concerns
The patient came to us with a pattern that I see often in this demographic: pigmentation that had been quietly worsening over time, with no clear single trigger and limited success with products tried at home. Specifically, the presentation included:
Diffuse melasma across the bilateral cheeks, chin, and perioral region
Uneven skin tone with a noticeable contrast between affected and surrounding areas
Mild sensitivity, particularly in the hyperpigmented zones, with a history of reactive responses to stronger active ingredients
Reduced confidence in her skin, which she mentioned directly at the first consultation
That last point matters. Melasma is not just a cosmetic concern. For many patients, it carries a real emotional weight, and that deserves to be acknowledged as part of the clinical picture.
Previous Treatment History
Prior to presenting at AMRÉ, no formal clinical treatment had been pursued for this concern. The patient had trialled a number of over-the-counter brightening products with results that were inconsistent at best. No laser, injectable, or naturopathic interventions had been used for this condition previously. This is actually quite common. Many patients arrive having spent months or years self-managing a condition that genuinely requires a more structured clinical approach to make meaningful progress.
Clinical Assessment
Understanding melasma means understanding that the skin is not misbehaving on its own. There is almost always something deeper driving the pigment response. My assessment process reflects that thinking.
Skin and Barrier Evaluation
Clinical examination confirmed epidermal melasma with bilateral symmetry, consistent with the patient's reported history of sun exposure and hormonal fluctuation. Importantly, the skin barrier in the affected zones showed signs of mild compromise, characterised by increased sensitivity and reduced tolerance to active ingredients. This was a key finding that shaped the entire protocol design. Introducing strong depigmenting agents into a compromised barrier does not accelerate results. It tends to provoke irritation, inflammation, and in darker skin tones, a risk of post-inflammatory hyperpigmentation that can worsen the very concern we are trying to address.
Contributing Factors
Based on a comprehensive intake, the following factors were identified as relevant contributors to the patient's pigment presentation:
Cumulative UV exposure without consistent sun protection as a primary driver
Hormonal influence, suggested by the distribution pattern and the patient's life stage
Elevated oxidative stress load based on lifestyle and dietary history
Prior use of actives that may have sensitised the skin without sufficiently targeting melanin regulation
Naturopathic Assessment
A thorough naturopathic intake was completed to evaluate systemic contributors to pigment dysregulation. I always want to know what is happening internally, particularly when it comes to antioxidant capacity, nutritional status, and the body's inflammatory burden. These are rarely discussed in a conventional aesthetics setting, but they matter enormously when you are trying to create lasting change in the skin. In this case, findings supported the addition of systemic vitamin therapy as a meaningful complement to the topical approach, targeting the biochemical pathways that drive melanin overproduction.
Treatment Protocol
I designed this as an ongoing, integrated protocol rather than a fixed endpoint plan. Melasma is a chronic condition, and managing it well means building something sustainable from the start, not just treating to a finish line. The two core pillars here were a structured topical skincare regimen and naturopathic intravenous vitamin therapy, introduced concurrently from day one. No laser or injectable treatments were incorporated in this case. That was a deliberate choice, not a limitation. For this patient's skin type, presentation, and barrier status, a conservative, well-sequenced approach was both appropriate and effective. The before and after images shared here reflect two months of consistent work. Progress has been meaningful, and the protocol continues.
Phase One: Skin Barrier Restoration
We did not start with actives. We started with the foundation. A two-week barrier restoration phase came first, and I would not skip this step regardless of how eager a patient is to begin treatment. A healthy skin barrier is what allows everything else to work.
A gentle, pH-balanced cleanser was introduced to preserve the skin's acid mantle. A ceramide-rich moisturiser was applied morning and evening to actively rebuild barrier integrity. Broad-spectrum SPF 50 or higher was established as a non-negotiable daily step from day one. All previous high-strength actives were paused to allow the skin to settle.
Two weeks of this foundation work made the skin ready to receive what came next.
Phase Two: Targeted Skincare Protocol
Once the barrier was stabilised, a stepwise active protocol was introduced. The ingredients were chosen for both their evidence base and their compatibility with the patient's skin type and sensitivity profile. Tyrosinase-inhibiting agents were introduced to reduce melanin synthesis at the source. Niacinamide was incorporated for its dual role in inhibiting melanin transfer and continuing to support barrier function. Azelaic acid was included for its anti-inflammatory properties and its suitability for sensitive or reactive skin. Vitamin C serum was added to the morning routine to neutralise UV-induced free radical activity and support overall skin radiance. SPF 50 or higher remained a daily commitment throughout.
The sequencing here matters as much as the ingredients themselves. Introducing too much too quickly is one of the most common reasons melasma treatments stall or backfire.
Phase Three: Intravenous Vitamin Therapy
This is where the AMRĒ approach becomes genuinely different from a standard aesthetics protocol. Intravenous therapy was initiated at the very beginning of the protocol, running concurrently with the skincare regimen from day one. While the topical regimen addressed pigment at the skin's surface, IV therapy allowed us to support the body's antioxidant defence and melanin regulation from within, at a level of bioavailability that oral supplementation simply cannot match.
Glutathione was the cornerstone of this component. It is one of the body's most powerful endogenous antioxidants, and its role in melanin modulation is well established. It works by inhibiting the conversion of eumelanin to phaeomelanin, shifting the skin toward lighter pigment production while simultaneously reducing the oxidative stress that drives melanogenesis. High-dose intravenous vitamin C was delivered alongside it, working synergistically to attenuate UV-triggered melanogenesis, support collagen synthesis, and reduce overall oxidative burden in the skin. B-complex vitamins were included to support cellular energy metabolism and encourage healthy skin cell turnover, rounding out the systemic component of the protocol.
Targeting melanin regulation through both topical and systemic pathways at once is what makes this protocol meaningfully different from surface-level management alone.
Phase Four: Homecare and Ongoing Maintenance
Compliance with homecare and sun protection is not optional when it comes to melasma. It is the variable that most determines whether a patient holds their results or continues to see improvement over time. I make this clear from the very first visit, and I revisit it at every follow-up.
The skincare routine was kept intentionally simple to reduce overwhelm and maximise consistency. Daily SPF was reinforced as the single most important step in the entire protocol. Physical sun protection measures were discussed, including protective clothing and seeking shade during peak UV hours. Because this is an ongoing protocol, regular reassessment appointments are built into the plan, allowing us to monitor progress, adjust as needed, and ensure the skin continues to respond well over time.

Figure 1: Clinical photographic documentation. Day 1 (baseline) and Month 2 (post-protocol). Shared with patient consent for educational purposes.
Clinical Outcome
Assessment Timeline: Eight weeks from protocol initiation
At the eight-week follow-up, the results were clinically meaningful and visually clear. Photographic comparison confirmed a significant reduction in melasma across the bilateral cheeks, chin, and perioral region. The pigment density had decreased noticeably, the skin tone was more uniform, and the overall complexion appeared smoother and more luminous. The patient reported feeling considerably more at ease in her skin, which, for me, is one of the most important outcomes of all.
Here is a summary of the documented clinical improvements:
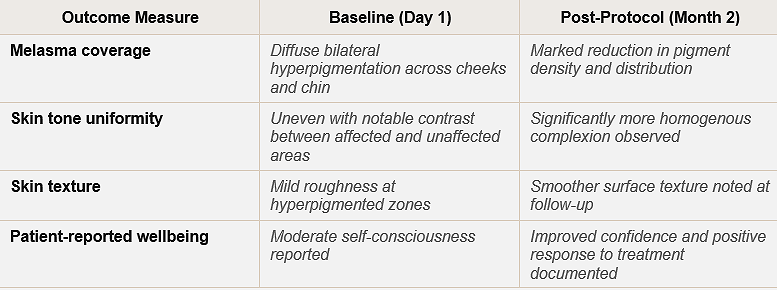
I want to be transparent about something. Melasma is a chronic condition. It can and does return, particularly with sun exposure or hormonal changes. What we achieved in eight weeks was a meaningful clinical improvement, not a permanent cure. Ongoing maintenance, consistent sun protection, and periodic reassessment are essential parts of the long-term plan.
Who May Benefit from a Similar Approach
Not every melasma patient will follow the same path. But if you recognise yourself in any of the following, a personalised assessment at AMRÉ may be a valuable place to start.
This protocol may be appropriate for individuals presenting with:
Epidermal or mixed melasma that has not responded adequately to over-the-counter brightening products
Fitzpatrick skin types III to VI, where more aggressive laser or chemical approaches carry a higher risk of post-inflammatory hyperpigmentation
A preference for a non-laser, lower-risk approach to pigment management
Systemic contributors such as hormonal imbalance or elevated oxidative stress that may be driving pigment overproduction
A history of barrier sensitivity or adverse reactions to high-strength actives
If you are unsure where you fall, that is exactly what a consultation is for. We assess first, then we plan. There is no guesswork involved.